Device-Based Therapy for Low Back Pain
, 2 years ago
Garima Anandani, MDT, CMP, DRPT1)*, Gautam M Shetty, MS Orth2),
Suraj Bafna, BPT, CMP1), Neha Narula, MPT1), Aabha Gandhi, BPT1)
1) Qi Spine Clinic: 301/B Jolly Bhavan 2, Next to Nirmal Niketan College, New Marine Lines, Mumbai
400020, India
2) Breach Candy Hospital, India
Abstract.
[Purpose] Device based therapy for
low back pain (LBP) involves quantitative assessment of muscle
strength, resistance and lumbar motion and tailoring the rehabilitation protocol based on this objective assessment.
The purpose of this study was to determine the effectiveness of device based therapy for LBP. [Subjects and Methods] In this retrospective study, clinical data of 235 patients who underwent device-based physiotherapy for low
back pain was reviewed. Pre and post-treatment outcome measures for pain (visual analogue scale or VAS score),
disability (Oswestry disability index) and functional ability were compared to determine effectiveness of devicebased physiotherapy at the end of 6 weeks of treatment. [Results] All outcome measures including VAS Score and
mean Oswestry Disability Score showed significant improvement at the end of 6 weeks of device-based physical
therapy. Before treatment, 73% of patients had moderate to severe disability which reduced to 28% after treatment.
[Conclusion] Device-based therapy is effective in relieving pain, improving function and reducing disability in
patients with low back pain in the short term. Device-based therapy may help to objectively evaluate the function of
the spine and paraspinal muscles and help the therapist tailor treatment accordingly.
Key words: Low back pain, Device-based therapy, Disability
Introduction
Low back pain (LBP) is one of the commonest musculoskeletal complaints and cause for disability globally1)
.
Conservative treatment or non-operative management which
includes physiotherapy is the main stay of treatment for nonspecific back pain whereas surgery is reserved for patients who have not shown any improvement with conservative management or in those where specific causes for the back pain or radicular pain has been identified2–4)
.
Physiotherapy has been reported to be effective in relieving LBP and involves a multidisciplinary approach aimed at
regaining function and preventing disability2–5)
. Physiotherapy regimes for management of LBP are varied and include
McKenzie lumbar spine exercises, intensive strengthening,
manipulation, device-based therapies, and low intensity
aerobics5–9)
. Device based therapy for LBP involves quantitative assessment of muscle strength, resistance and lumbar
motion and tailoring the rehabilitation protocol based on this
objective assessment.
Although several reports have analysed the effectiveness of standard physiotherapy for LBP, literature is lacking in
terms of effectiveness of device based therapy for LBP.
To the best of our knowledge, there are no studies in the
literature which have reported effectiveness of device based
therapy for LBP. Hence, the purpose of this study was to
determine the effectiveness of device based therapy for LBP
Subjects And Methods
We retrospectively reviewed the clinical records of patients treated for low back pain (LBP) using device-based
physical therapy during a 1 year period between March 2013
and March 2014. The inclusion criteria were device-based
physical therapy done for patients with low back pain where
red flags (Fever, Recent trauma, Pain at night or at rest, Progressive motor or sensory deficit, Saddle anaesthesia, Unexplained weight loss, History of cancer or strong suspicion
of cancer, History of osteoporosis or chronic steroid use,
Immunosuppression, Failure to improve after 6 weeks of
conservative therapy) were ruled out using clinical history,
examination and magnetic resonance imaging (MRI)10, 11)
.
The exclusion criterion was incomplete clinical records
where demographic and clinical outcome data could not be
obtained. Based on the inclusion criteria, clinical records of
250 patients were available for review. Fifteen patients had
to be excluded due to incomplete records leaving 235 patient
records for analysis.
Before induction into therapy, every patient underwent
detailed assessment by a therapist which included taking
down detailed history, a thorough clinical examination and
review of their MRI report. Demographic details such as
age, gender, height, weight, body mass index (BMI), and
lifestyle and clinical history details such as duration of back
pain, number of previous episodes, past history of trauma
or surgery, pain radiation was obtained from the clinical
records. The clinical examination included assessment of
posture, lumbar spine movement loss and flexibility, neurological and motor/myotome examination. Pain before
and after treatment was recorded using the Visual Analogue
Scale (VAS) system. Functional disability before and after
treatment was recorded using the Oswestry low back pain
disability score12)
.
The device-based physical therapy program followed a
standardised protocol including 18 sessions spread over 6
weeks. The program was provided by physiotherapists based
at 2 centres. The program began with pain control regime
combined with the McKenzie lumbar spine exercises. The
purpose was to reduce the pain so that the patient can then
be put on the device for objective assessment of lumbar
spine movement loss and flexibility and paraspinal muscle
strength and endurance using the David Spine Concept
system (David Health Solutions, Helsinki, Finland). This
machine is equipped with a knee-lock system and a thighrestraining belt to immobilize both hips and thighs which
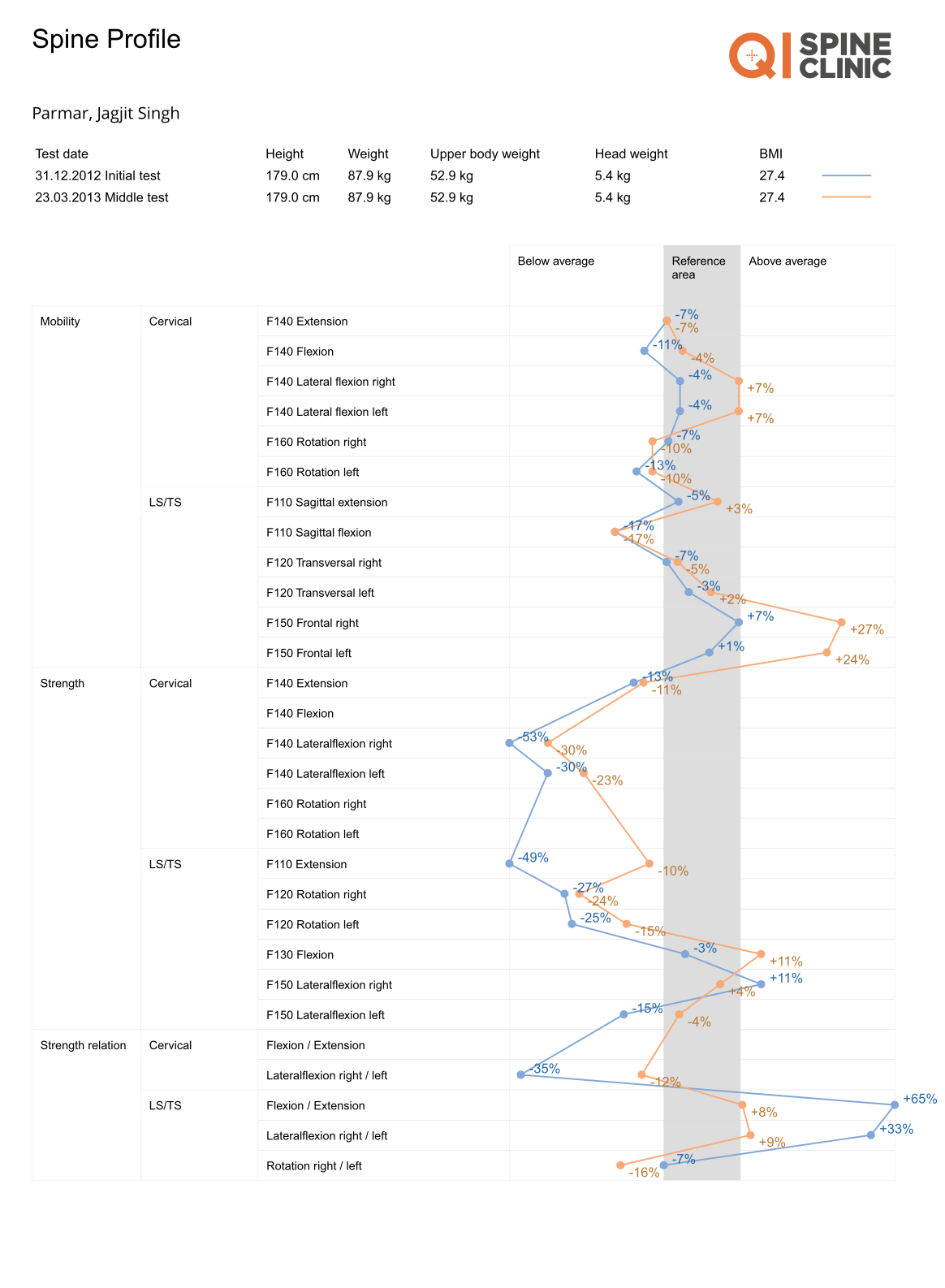
allowed the patient to move only the lower back. The patient
was then put on a customised protocol based on the readings of the device which was plotted on a graph called the
Digital Spine Analysis (DSA) Graph. The program aimed to
increase both strength and endurance of the back/paraspinal
muscle with 15 to 20 repetitions every session on the device.
If the patient was able to perform more than 20 repetitions of
slow and controlled back extension and flexion movements,
2–2.5 kg was added in the next training session. However,
if the patient was able to perform less than 15 repetitions,
the training load was lowered by 2–2.5 kg next time. Post
treatment outcome measures such as VAS Score, Oswestry
Score and category and Functional ability were all recorded
after completion of 6 weeks of physical therapy.
The pre and post treatment (at the end of 6 weeks of
device-based therapy) outcome measures of VAS Score,
Oswestry Score and Functional ability were compared using
the Student’s t-test for continuous data and Fisher’s exact
test for categorical data. A p value of <0.005 was considered
significant.
Results
There were 142 male patients and 93 female patients
with a mean age of 44±13.8 years (range, 17–84 years) and
a mean BMI of 26.5±4.3 (kg/m2). One hundred and seventytwo patients reported to lead a sedentary lifestyle and 63
patients had a semi-active to active lifestyle. The duration of
low back pain ranged from days to years and the most common lumbar spine level affected on MRI was L4-S1 level.
The common pathological changes reported on lumbar MRI
included disc bulge, disc protrusion, disc herniation, facetal
arthropathy, spondylolisthesis and canal stenosis
All outcome measures showed significant improvement
at the end of 6 weeks of device-based physical therapy. Low back pain as measured by the mean VAS score reduced
significantly from 4.8 to 0.6 (p=0.0001) whereas the mean
Oswestry score improved from 39 to 15.3 (p=0.0001) after
treatment. Before treatment, 73% of patients had moderate
to severe disability owing to their low back pain whereas
after treatment this number dropped down to 28%. Similarly, the functional ability to perform daily tasks such as
sitting (33% vs. 85%), standing (31% vs. 81%) and walking
(29% vs. 85%) also improved significantly after treatment
(p=0.0001).
Discussion
The current study sought to determine the effectiveness
of device-based physical therapy for treatment of low back
pain. Patients in our study showed significant reduction in
VAS Score for pain and Oswestry disability score and improvement in functional ability thus confirming that devicebased therapy is quite effective in relieving pain, improving
function and reducing disability in patients with low back
pain in the short term.
The David Spine Concept system (David Health Solutions, Helsinki, Finland) used in this study acts as a diagnostic tool and allows the therapist to determine functional
deficit of the lumbar spine which includes restriction of lumbar motion and strength of the paraspinal muscles. Hence,
this device-based protocol helps the therapist to identify
functional deficits in each individual and tailor his treatment
accordingly.
Literature is lacking for reports on the effectiveness of
device-based therapy for conservative management of low
back pain. Helmhout et al.12)
conducted a randomised controlled trial in military recruits to determine the effectiveness
of device-supported specific lumbar extensor training compared with regular physical therapy in subjects with nonspecific, nonacute LBP. They reported that device-supported
specific back strengthening did not offer greater benefits
when compared to routine physiotherapy in the treatment
of LBP12)
. However, their study population had stricter
inclusion criteria and had recruits with similar background
whereas our study population showed greater variability in
terms of age, gender and lifestyle. Furthermore, the devicesupported therapy used in the study by Helmhout et al.12)
involved specific lumbar extensor strengthening only unlike
the treatment protocol in our study which was varied based
on variability in strength, motion and function as highlighted
by the David Spine Concept system.
There are a few limitations to our study. First, the retrospective design of this study has its own limitations and
inherent biases. Second, the results reported are at the end
of 6 weeks of therapy and the long term implications or effectiveness of device-based therapy in the management of
LBP is not known and needs to be studied further. Finally,
a well-designed, prospective randomised trial needs to be
undertaken to further confirm the benefits and advantages
of device-based therapy over regular physiotherapy for the
conservative management of LBP.
In conclusion, device-based therapy is quite effective in
relieving pain, improving function and reducing disability in
patients with low back pain at the end of 6 weeks of therapy.
Device-based therapy may help to objectively evaluate the
function of the spine and paraspinal muscles and help the
therapist tailor treatment accordingly.
References
- 1) Vos T, Flaxman AD, Naghavi M, et al.: Years lived with disability (YLDs)
for 1160 sequelae of 289 diseases and injuries 1990–2010: a systematic
analysis for the Global Burden of Disease Study 2010. Lancet, 2012, 380:
2163–2196. [Medline]
- 2) Koes BW, van Tulder M, Lin CW, et al.: An updated overview of clinical
guidelines for the management of non-specific low back pain in primary
care. Eur Spine J, 2010, 19: 2075–2094. [Medline]
- 3) Peul WC, Bredenoord AL, Jacobs WC: Avoid surgery as first line treatment for non-specific low back pain. BMJ, 2014, 349: g4214. [Medline]
- 4) Chou R, Baisden J, Carragee EJ, et al.: Surgery for low back pain: a review
of the evidence for an American Pain Society Clinical Practice Guideline.
Spine, 2009, 34: 1094–1109. [Medline]
- 5) Hayden JA, van Tulder MW, Malmivaara A, et al.: Exercise therapy for
treatment of non-specific low back pain. Cochrane Database Syst Rev,
2005, 3: CD000335. [Medline]
- 6) Chou R, Huffman LH, American Pain Society American College of Physicians: Nonpharmacologic therapies for acute and chronic low back pain: a
review of the evidence for an American Pain Society/American College of
Physicians clinical practice guideline. Ann Intern Med, 2007, 147: 492–
504. [Medline]
- 7) Mannion AF, Müntener M, Taimela S, et al.: Comparison of three active
therapies for chronic low back pain: results of a randomized clinical trial
with one-year follow-up. Rheumatology (Oxford), 2001, 40: 772–778.
[Medline]
- 8) Lee W, Lee Y, Gong W: The effect of lumbar strengthening exercise on
pain and the cross-sectional area change of lumbar muscles. J Phys Ther
Sci, 2011, 23: 209–212.
- 9) Lee JS, Yang SH, Koog YH, et al.: Effectiveness of sling exercise for
chronic low back pain: a systematic review. J Phys Ther Sci, 2014, 26:
1301–1306. [Medline]
- 10) Lateef H, Patel D: What is the role of imaging in acute low back pain? Curr
Rev Musculoskelet Med, 2009, 2: 69–73. [Medline]
- 11) Chou R, Qaseem A, Snow V, et al. Clinical Efficacy Assessment Subcommittee of the American College of Physicians American College of Physicians American Pain Society Low Back Pain Guidelines Panel: Diagnosis
and treatment of low back pain: a joint clinical practice guideline from
the American College of Physicians and the American Pain Society. Ann
Intern Med, 2007, 147: 478–491. [Medline]
- 12) Helmhout PH, Harts CC, Viechtbauer W, et al.: Isolated lumbar extensor
strengthening versus regular physical therapy in an army working population with nonacute low back pain: a randomized controlled trial. Arch Phys
Med Rehabil, 2008, 89: 1675–1685. [Medline]